
Complete Guide to HCC Risk Adjustment in Medical Coding
Discover expert strategies to maximize HCC Risk Adjustment accuracy, improve coding efficiency, and ensure better patient care outcomes.
Medicare Advantage has been at a critical crossroad. By January 1, 2026, the three-year transition to the new version 28 (V28) of the CMS Hierarchy Condition Category model version 24 (V24) is done. Numbers 100% of risk adjusted payment are currently computed under the V28 model only, and not on any other payment year than 2026. This is not a technical update. It represents a radical change in the documentation, coding and valuation of chronic disease.
Learning the art of HCC risk adjustment in the fully operationalized V28 system is crucial to revenue cycle integrity, regulatory compliance, and financial sustainability in the case of medical coders, billers, and practice managers. This is the full Billing Care Solutions guide to HCC risk adjustment, with the ultimate roadmap to get you through 2026 and beyond.
Introduction to HCC Risk Adjustment in 2026
What is HCC Risk Adjustment?
The Hierarchy Condition Category model is a type of risk adjustment framework applied by Centers of Medicare and Medicaid services to estimate future healthcare expenses of beneficiaries with regard to their health conditions. The payment HCC categories in place under the new V28 model have grown to 115, with 86 becoming 115; the new model is able to capture the complexity of patients in a much more detailed way. This expansion however had a major trade off, more than 2,200 codes of diagnosis were dropped completely off the payment model . This implies that numerous ambiguous or undefined codes which previously were associated with an increased risk score are no longer assigned to any HCC within V28.
The 2026 Landscape: Full Implementation of V28
The Transition is Complete:
The phase in period is over. In payment year 2026, CMS will compute the HCC risk adjustment scores based on the V28 model only. The mixed strategy consisting of V24 and V28 is concluded. CMS has revaluated the final V28 model with the latest available data, namely, diagnoses in 2022 and cost data in 2023 and released the final risk adjustment coefficients and the predicted ratio table of all factors to be effective in this payment year.
What Full V28 Means for Coders
V28 requires a higher degree of clinical specificity of providers and coders to be in place. The once general code conditions must be documented in detail.
In the case of V24, one could have just stated that they had heart failure. The claim must contain the information of ejection fraction percentage, acute or chronic, systolic or diastolic clarification if the person is below V28. These clinical indicators are no longer to be added retrospectively, they have to be recorded at the point of care. Real time accuracy is the central element of successful HCC risk adjustment in 2026.
The Building Blocks: How HCC Risk Adjustment Works in 2026
From ICD-10 to HCC:
The documentation of the provider will start this process. A coder will encode the condition of a patient into a certain ICD-10-CM code. The code then gets mapped to one of the 115 payment HCC categories of the V28 model . It is also important to keep in mind that thousands of codes were deleted during transition; application of an outdated or unspecified code could lead to the overall failure of any HCC being recorded.
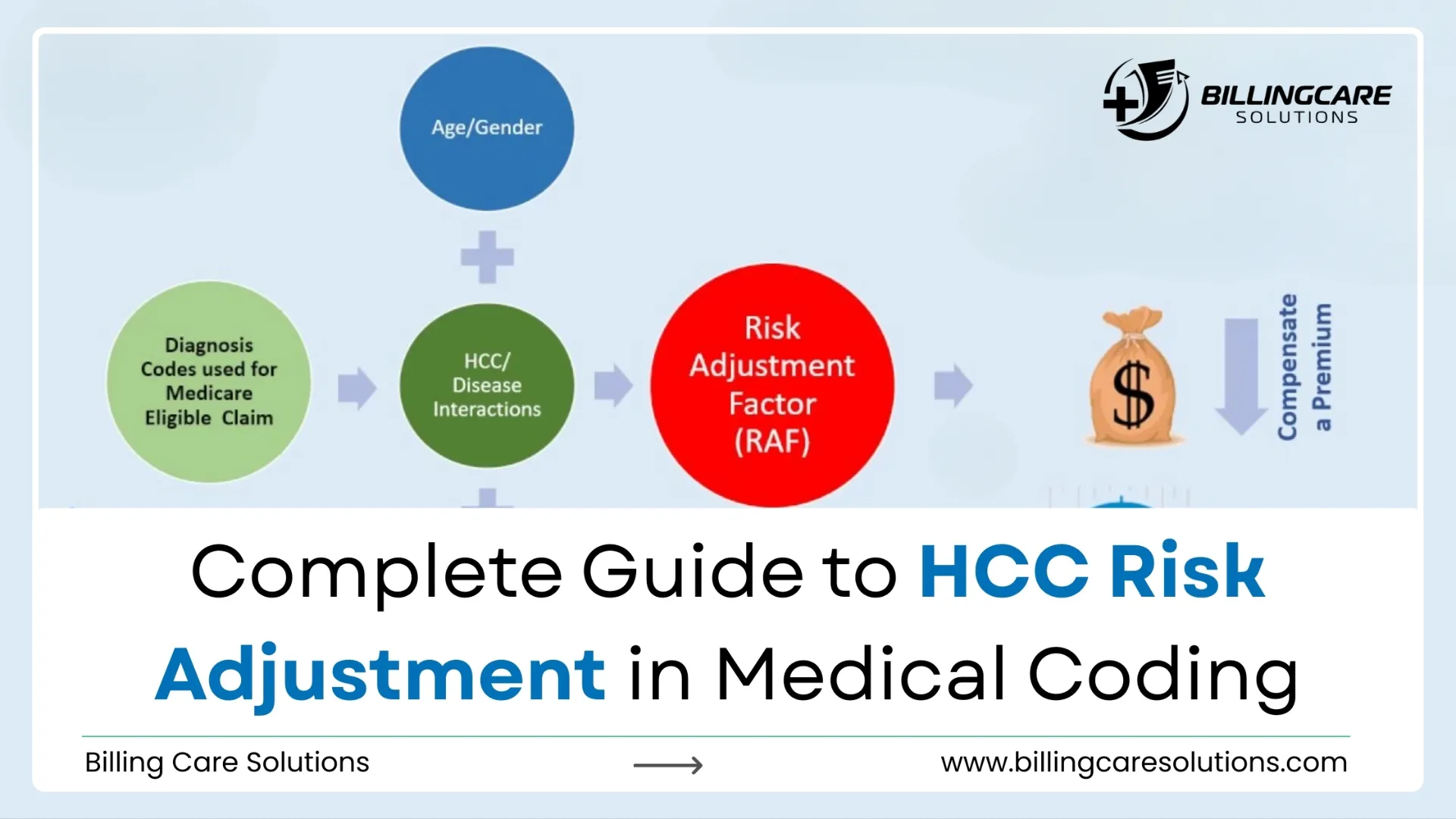
Understanding RAF Scores:
The RAF score of a patient is obtained by summing the demographic variables such as the age, gender, and Medicaid status of the patient with the disease coefficients of the mapped HCCs. Beneath V28, CMS created a notion known as a constraining, where in some categories of diseases the HCC score is equal irrespective of the problematic expenses or issues of the diseases. This further increases the accuracy of capture of unique, non constrained conditions as even more important towards constructing accurate RAF scores.
Disease Interaction Terms:
The treatment of the terms of interaction of the diseases is one of the most significant subtleties of the V28 model. The terms of interaction within the CMS-HCC model are additive and are independent of HCC hierarchy. It implies that although one of the diagnoses in an interaction pair, such as diabetes and congestive heart failure, may be trumped, by a more severe HCC in the same group, the interaction term is still factored in the risk score of the patient. Strategic HCC risk adjustments is recognizing such high value condition pairs so that they are identified every year.
Best Practices for Accurate HCC Risk Adjustment Coding Under V28
Mastering the MEAT Criteria:
The MEAT(Monitor, Evaluate, Assess/Address, Treat) criteria is the gold standard of documentation. Each diagnosis presented to risk adjustment shall be of Monitoring, Evaluating, Assessing, or Treating the condition in a face to face presentation. A condition mentioned in the history of a patient but not actively treated within the past year should not be risk adjusted. This is the best standard you have against a Risk Adjustment Data Validation audit.
The Importance of Specificity:
Specificity is the force that drives the correct RAF scores to be made below the 2026 model. Documentation that connects conditions with granular detail has to be sought out by coders. General codes of vascular disease, nutritional disorders and some kidney conditions are reclassified so that they need very high levels of documentation to attract a payment. When your clinical records are still used in 2026, with the same number of patients, your income will decrease, even though the code is still 2024.
Managing the Problem List:
The Electronic Health Record lists the issue within the patient and should be accurate and up to date. This list should be reconciled against clinical notes by coders and providers on a regular basis to make sure that all chronic conditions are consistent with the V28 specificity criteria and that they are corrected. The first line of defense in successful HCC risk adjustment is a clear, focused list of problems.
Proactive vs. Retrospective Risk Adjustment in 2026
The Shift to Prospective Risk Adjustment:
As V28 is fully implemented and CMS is looking more closely at the industry, it is moving away from retrospective chart chasing. The standard of care has changed to prospective HCC risk adjustment. This entails the recognition and the capture of all the pertinent diagnoses in the patient encounter. This is done by conducting pre visit chart reviews, EHR alerts, which remind the providers to make certain documentation, and intake forms, which are used to identify possible gaps. Recording the appropriate codes at the point of care saves on the administrative cost of fixing the coding afterwards and provides the complete picture of the health of the patient to the provider.
The Future of Retrospective Review:
The role of the retrospective review is altering. Suggested laws such as the so-called No UPCODE Act would prohibit the use of diagnosis codes that are received based on chart reviews and health risk assessment to generate payment, which would effectively remove the retrospective review as a technique to amend missing coding. Although this trend is not yet enforced, it is important to note that getting it right the first time is necessary. The existing retrospective activities must be directed towards audit defense and finding education opportunities to the providers, as opposed to seeking revenue recovery through them.
The Role of Technology in Modern HCC Risk Adjustment
AI and Natural Language Processing:
The amount of information and the specifics demanded by V28 are too large to be reviewed by hand. The coding processes are being changed by technology namely the Natural Language Processing. NLP has the ability to scan physician notes as they are typed, and point out conditions and areas where more specificity should be applied to allow the risk to be captured successfully. These AI based applications are capable of giving real time coding suggestions in the point of care without affecting the workflow of a physician.
Real Time RAF Scoring:
Contemporary systems are able to compute RAF score impact in real time when a patient is being attended to. This will enable the providers to observe the financial as well as the clinical relevance of the diagnoses they are recording, which underlines the relevance of thorough and definite notes. These tools can assist in the bridging of the gap between clinical documentation and risk scoring through the incorporation of clinical data and terminology maintenance along with coding support.
How Billing Care Solutions Can Help?
It is hard to find an easy way out of the complications of the fully developed V28 model without the help of a dedicated partner. Billing Care Solutions is a company that deals in end to end HCC risk adjustment. Our certified coders are only trained on CMS-HCC V28 model and thus your coding is accurate, compliant, and is optimized to the current payment year.
We provide both prospective CDI support services as well as retrospective audit defense services as per the needs of your organization. Through our association, you will have an extension upon your team that would work on enhancing RAF precision, audit threat and revenue cycle streamlining. We keep abreast with regulatory changes to enable you to attend to patients.
Conclusion:
The era of V28 is here. As 100% of risk scores are now computed using the new model, the only way to go to fiscal health and compliance is precision of HCC risk adjustment. Those organizations investing in sound documentation practices, utilizing technology, and collaborating with experts in the field of coding will succeed, as they would be adequately rewarded due to the complexity of care they offer. The retrospective fixes timeframe is running out; now is the time to create a prospective, valid coding workflow.
Are you willing to maximize your risk adjustment program in the V28 age? Call the Contact Billing Care Solutions now to get a consultation. Allow our specialists to assist you in realizing the most of the care you provide and remain audit ready and compliant.
